
NREMT Skillset/Physiology of Blood Pressure
| Parent | Blood Pressure Auscultation |
|---|
The Heart
[edit | edit source]The heart is divided into four major chambers, two atria and two ventricles. The left ventricle is responsible for the pulse we feel and the arterial blood pressures we assess in the field as EMTs and paramedics. Blood moves from the atria to the ventricles in sequential beats: the atria (top two chambers) squeeze, or "beat", in conjunction which moves the blood they contain to the more muscular ventricles (bottom two chambers). The ventricles then "beat" in conjunction with each other and force the blood out of the heart.
An easy way to remember the difference between atria and ventricles is that the atria (singular: atrium) are the entryways to the heart, similar to how an atrium is the entryway to a building; therefore, blood enters the heart via the atria. The ventricles similarly vent blood out of the heart; therefore blood leaves the heart through the ventricles.
Diastole is when the ventricles are at rest and are being filled by the atria while systole is when the ventricles contract and force blood out of the heart, creating a palpable pulse in a healthy person.
Arteries and Veins
[edit | edit source]Arteries are the muscular blood vessels that carry blood away from the heart and to the body's tissues. Their muscular walls allow for vasoconstriction or the narrowing of the artery in response to external or internal factors and vasodilation or the relaxation of the aforementioned constriction. This allows for shunting of blood away from areas of the body that do not need it and towards areas of the body that need more blood.
In contrast, veins carry blood towards the heart and are structurally very different than arteries. Both arteries and veins are tubular, but veins lack the muscular tunica media that arteries possess. Instead, veins are often large and easily collapsible. Additionally, veins possess one-way valves which prevent retrograde flow of blood. Veins move blood through a slow buildup of pressure or gravity. This slow process can be sped up by rhythmic contraction of the muscles surrounding the veins, essentially "squeezing" the blood from a one-way valve past another until the blood reaches the heart again.
Overview of Blood Pressure
[edit | edit source]Blood pressure is one of the vital signs EMTs are expected to be proficient in assessing and is used at all levels of medical care from initial patient contact in the prehospital environment all the way through hospital discharge and possibly beyond. Adequate blood pressures allow for adequate perfusion of the body tissues, meaning that oxygen and nutrient levels are sufficient for the level of metabolic consumption that specific tissue is undergoing at that moment. Blood pressure is measured in mmHg (millimeters of mercury that would be displaced by this amount of atmospheric pressure in a barometer at sea level). A patient is generally considered to be in shock if their systolic blood pressure is below 90 mmHg. Shock is a potentially life threatening condition where important tissues such as the brain, heart, lungs, and other vital organs may be hypo-perfused.
Blood pressure readings are comprised of two numbers, the systolic and diastolic. In a blood pressure reading, the systolic blood pressure is found on the top (e.g. 120/80) while the diastolic blood pressure is found on the bottom (e.g. 120/80). Each of these numbers relates directly to pressure in the arteries. A venous pressure is more difficult to obtain as the veins are low pressure systems and move blood primarily through one-way valves and a combination of skeletal muscular contraction, gravity, and pressure.
Arterial Blood Pressure
[edit | edit source]Arterial blood pressures are the most commonly monitored and are the only blood pressures able to be monitored in the field by an EMT or paramedic without significantly advanced monitoring (i.e. something like a Swan-Ganz Catheter, which is not normally able to be inserted prehospitally at this time). There are two types of easily manually assessed arterial pressures, auscultated and palpated. Auscultated blood pressures are performed with a sphygmomanometer (i.e. blood pressure cuff) and a stethoscope and rely on the provider "auscultating", or hearing, the return of blood flow and loss of Kortotkoff sounds. Palpated blood pressures are performed with only a blood pressure cuff and rely on the provider feeling the return of blood flow by palpating a pulse point. Automated or mechanical blood pressures are may also be obtained; these generally use oscillations in pressure rather than sound to obtain a blood pressure. Additional blood pressure measurements may be made through arterial lines which are inserted by skilled providers directly into the lumen of an artery; these are rare to find in the prehospital environment but provide a beat-by-beat real-time look a the patient's blood pressure. As mentioned earlier, systolic blood pressure is the pressure found in the arteries when the heart is beating, while diastolic blood pressure is the pressure in the arteries when the heart is at rest.
Venous Blood Pressure
[edit | edit source]This will be a quick overview of venous blood pressure as it is not normally obtainable in a prehospital environment. Venous pressures are much lower than arterial pressures, normally sitting around 2-6 mmHg. This much lower pressure means that venous pooling can be an issue if the patient is at rest or sedentary for long periods of time; this pooling and stagnant blood can clot and lead to DVTs and other complications. Venous blood pressures can only be monitored with advanced, invasive devices and are not normally used in the prehospital environment.

Palpated Blood Pressure
[edit | edit source]The palpated blood pressure is obtained by inflating the blood pressure cuff while simultaneously palpating a pulse point distal to the cuff, the radial artery is the most commonly used pulse point for this purpose. As the artery is compressed between the provider's fingertips and bone, blood flow can be interrupted and creates the tactile "pulse" as the heart beats. If a pulse point is subjected to too much pressure (i.e. a higher pressure than the patient's systolic blood pressure), no pulse will be palpated. As the pressure of the blood pressure cuff reaches the patient's systolic blood pressure, blood passes beyond the boundary of the cuff and moves distally where it can be felt by the provider. Because palpation by definition is an interruption of normal laminar flow (discussed later), only the systolic blood pressure of the patient can be obtained by palpation: therefore palpated blood pressures are noted as "SYSTOLIC/P".
Automated and Auscultated Blood Pressure
[edit | edit source]Laminar and Turbulent Blood Flow
[edit | edit source]-
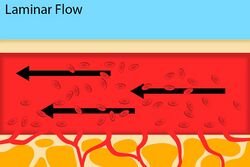 Fig. 2: Normal blood flow through an artery.
Fig. 2: Normal blood flow through an artery. -
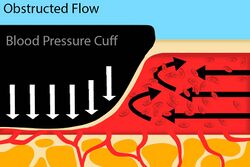 Fig. 3: An artery with a blood pressure cuff where the cuff pressure is greater than the systolic blood pressure.
Fig. 3: An artery with a blood pressure cuff where the cuff pressure is greater than the systolic blood pressure. -
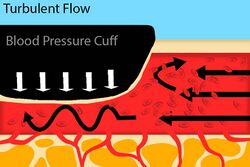 Fig. 4: An artery with a blood pressure cuff where the cuff pressure is less than the systolic, but still greater than the diastolic blood pressure.
Fig. 4: An artery with a blood pressure cuff where the cuff pressure is less than the systolic, but still greater than the diastolic blood pressure.



Laminar flow is defined as a flow pattern where all of the fluid particles are moving in parallel lines. This type of flow pattern is seen when arteries are fully open and are not compressed. If a stethoscope is used to auscultate this artery, there would be no sound as the blood is not "colliding" with anything as it travels in parallel lines. Laminar flow is seen in Figure 2.
Turbulent flow is defined as a flow pattern where the fluid particles undergo random movement, creating mixing. This type of flow pattern is seen when arteries are compressed. In Figure 3, blood flow is turbulent because of the obstruction, but no sound would be able to be auscultated beyond the blood pressure cuff because there is not blood flow distal to the cuff. In Figure 4, blood flow is still turbulent, but with one significant difference: there is blood flow distal to the blood pressure cuff, meaning that Kortotkoff sounds would be able to be auscultated.
Auscultated Blood Pressure
[edit | edit source]Auscultated blood pressure is taken by inflating a blood pressure cuff and placing a stethoscope over an artery and distal to the cuff. The blood pressure cuff is inflated past the systolic blood pressure obtained by palpation or until a pulse can no longer be heard. The cuff pressure is then slowly lowered until Kortotkoff sounds can once again be auscultated; this is the systolic blood pressure. The cuff pressure is continually lowered until there is a loss of Kortotkoff sounds, indicating that the artery remains fully patent despite the pressure of the cuff; this point is the diastolic blood pressure.
The systolic blood pressure produces Kortokoff sounds as the pressure of the cuff shifts from Figure 3 to Figure 4. As the heart beats, the artery experiences enough pressure to overcome that of the cuff and allow for movement of blood past the cuff. This blood's flow is turbulent, and creates an audible sound. Because the cuff pressure is still higher than the diastolic blood pressure, the artery will once again collapse under the pressure of the cuff during diastole (when the heart is at rest and no longer providing increased pressure in the arteries). Although it may not fully close, the deviation in the arterial walls is enough to still produce turbulent flow. As the blood pressure cuff's pressure lowers, the artery will collapse less and less, until it remains fully open throughout the whole cardiac cycle.
The diastolic blood pressure marks the loss of audible "whooshes" or "beats" because there is enough residual pressure left in the artery during diastole (cardiac rest) to fully overcome the pressure of the blood pressure cuff. This means that the artery looks like Figure 2 and regains laminar flow, which is relatively soundless since the blood is not "bumping" into anything on its way through the artery.
Automated/Mechanical Blood Pressure
[edit | edit source]Automated or mechanical blood pressures are obtained by instruments like cardiac monitors or automated blood pressure cuffs. These machines are often useful as they allow the provider to automatically collect trending sets of blood pressures or perform other tasks while blood pressure monitoring is in progress. Despite their usefulness, these machines are susceptible to several potential failures which would result in an inaccurate blood pressure reading. Because there is no thinking person at the "other end" of the machine, these failures can easily be overlooked by providers if they are not careful. A brief overview of some of the most common failures will be provided after this discussion on how the blood pressure is obtained.
After the cuff is placed on the patient, the machine inflates the cuff with air. This inflation step is identical to the inflation of a manual blood pressure cuff, and the internal cuff pressure is constantly measured by a digital pressure gauge. As the patient's heart beats, their arteries expand slightly and push against the pressure provided by the cuff; this provides a small, but measurable, increase in the internal pressure of the cuff. The automated machine reads this pressure and keeps inflating until there is no longer a pulsatile increase in pressure (i.e. the cuff pressure is higher than the systolic blood pressure). Once the machine has narrowed in on a systolic blood pressure, it slowly lowers the cuff pressure until the pulsatile pressure increases are no longer detectable; at this point the diastolic blood pressure is capable of maintaining a full lumen and the cuff pressure does not produce any additional turbulent flow.
Common issues with this type of blood pressure monitoring come from interference with the pressure monitoring, either from the patient or the provider. These machines often come with multiple sizes of cuff, and an incorrectly sized cuff can lead to artificially high or low pressures if it is too small or large, respectively. Additionally, if the patient is moving and/or tensing their muscles, the machine may read those subsequent increases in pressure as systolic contractions and increase the cuff pressure to overcome the "false systole". This can be intensely uncomfortable for the patient as the cuff continues to "squeeze" and can lead to falsely elevated readings or even machine "time-out" where the machine is unable to obtain the blood pressure in a set amount of time and cannot display a reading.
| Authors | Global Surgical Training Challenge |
|---|---|
| License | CC-BY-SA-4.0 |
| Cite as | JHantke (2021–2025). "NREMT Skillset/Physiology of Blood Pressure". Appropedia. Retrieved July 29, 2026. |