

The GlobalSurgBox, the Universal Surgical Simulator that fits in a toolbox, is a surgical simulator that fits in a 12.5-inch toolbox, is capable of teaching trainees valuable surgical skills such as: knot tying, basic and advanced suturing, bowel and vascular anastomoses, aortic valve replacement, and numerous other new and emerging possibilities.
This simulator has been put into use in settings all over the world, including Kenya, Rwanda, and the USA.
What problem are we aiming to solve?[edit | edit source]

The importance of simulation in surgical training is widely acknowledged. Simulation training has been shown to decrease operative time, increase accuracy, and help with management of adverse events and produce safer surgeons.1,2 In low-resource environments, training opportunities can be far more limited than in high-income settings, rendering simulation training especially valuable.3,4
Despite these known benefits, current simulation platforms are limited by multitude of barriers, including affordability, portability, accessibility, and ease of implementation into existing training programs. Simulation centers are often very expensive, with costs reported at estimated at $876,485 for set up (renovation of existing facility, equipment) or $110,300-$361,425 for annual operation5,6. This is a significant barrier for educational institutions in low- and middle-income countries (LMICs).
We have created a solution to these barriers by designing a low-cost, adaptable surgical simulator to overcome resource constraints, allowing for easy and affordable implementation. Assembled from common supplies gathered in one’s home or local stores, our simulators enable trainees to practice a variety of skills regardless of their location, academic affiliation, time constraints, or resource stratum. By decreasing many of the previously stated barriers to practice, these have powerful implications especially in global health settings.7,8,9
The goal of our simulator is to allow surgical trainees to become confident and competent in performing a variety of surgical techniques as part of a self-driven surgical simulation training curriculum. Through the development of these surgical technical skills, trainees are able to demonstrate proficiency in the operating room and take on progressive responsibility for performing the surgical procedure. This is especially important for making the most of their training and for providing excellent quality of care to their patient.
Simulation[edit | edit source]
The GlobalSurgBox was designed on the principles of:
(1) accessibility, (2) adaptability, (3) affordability, (4) autonomy
(1) Accessibility[edit | edit source]
The GlobalSurgBox is a surgical trainer that is housed entirely within a 12.5-inch toolbox. The lid of the toolbox has built-in compartments to store sutures, nails, and other supplies. Inside the toolbox, a removable tray contains the necessary surgical instruments including needle drivers and forceps. At the base of the toolbox, a wooden board serves as the foundation for all surgical training exercises (Figure 1).
Our design eliminates the need for expensive or cumbersome simulation technologies, and the need for complicated set up routines. Traditional surgical simulation usually happens in a simulation center, often in a separate building from a trainee's workplace, with need to schedule specific times for practice that are often inconvenient for the trainee.
The portable nature of our simulation trainer means trainees can perform drills anymore, whether it be one's home, or easily be transported back and forth to the hospital. Trainees can also practice with limited timeframes: while a patient is being prepared for surgery by the anesthesia team, or while waiting for a patient to stabilize in the ICU postoperatively. When a resident asks their senior trainee or attending how a skill or technique is done, the simulator can be optimized for a brief demonstration. The nature of the GlobalSurgBox truly allows for independent or guided practice in any setting, which we strongly believe encourages more practice and skill development.
(2) Adaptability[edit | edit source]
The GlobalSurgBox is adaptable to any resource setting or country, as well as any skill level of its user.

The GlobalSurgBox has been used by trainees at all levels of training, from the medical student, general surgery resident, to the cardiothoracic or vascular surgery fellow. By using strategically placed nails on a common board (Figure 2A), an infinite number of exercises can be designed to fit the needs and skills of the user. The simulator can also grow with the trainee: once they have mastered basic skills (knot tying, basic suturing skills), they can move on to more advanced techniques (CABG, anastomosis) with the exact same tool. A few of our modules are listed here:
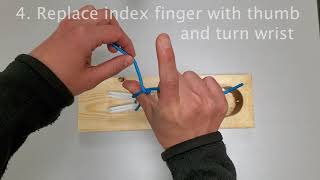
- Knot Tying (Figure 2B)
- Two-handed knot tying, one-handed knot tying (Tutorials for these have been created here - https://globalsurgbox.com/436-2/)
- Slip knot vs square knots, tying in a "hole", instrument ties
- Basic Suturing Skills (Figure 2C)
- Basic Suturing, Baseball stitch, Horizontal Mattress Stitch (Tutorial created here - https://globalsurgbox.com/436-2/)
- Vascular Anastomoses (Figure 2C)
- End-to-end, end-to-side, vascular patch repair
- Bowel Anastomoses
- End-to-end, end-to-side, side-to-side
- Advanced Coronary/Vascular Skills (Figure 2D)
- Coronary bypass graft - proximal anastomosis (Tutotial created here - https://globalsurgbox.com/475-2/)
- Coronary bypass graft - distal anastomosis
- Aortic Valve Replacement
- Tendon repair, inguinal hernia repair, and many others!
The GlobalSurgBox is also adaptable to any setting or country. So far, it has been used in training institutions and medical schools in Rwanda, Kenya, and multiple states in the USA. We foresee that learners and trainers will be able to continue to innovate and create modules based on the supplies that are available in their specific setting as well as their own training needs. For example, in the USA, the kit utilizes yoga mats for suturing practice, whereas in Kenya, flip flops are being used for the same exercises due to their ubiquity and interchangeability. Our modular design encourages crowdsourcing of new ideas, which we plan to disseminate through an online forum.
(3) Affordability[edit | edit source]
The GlobalSurgBox is designed to be extremely affordable. The entire simulator with a full set of materials can be assembled for $20 USD. All supplies can be found online or in local stores, which means that trainees are no longer reliant on mentors to provide them with materials for practice. This also encourages trainees to continuously find better and more affordable alternatives based on local needs and availability. This not only expands ideas for the GlobalSurgBox, but encourages use by students and reinforces reproducibility. With the ability to create their own box and replenish supplies at any time, practice never has to stop.
(4) Autonomy[edit | edit source]
For far too long, training and simulation has been dependent on too many factors, including a mentor's availability or sometimes even their mindset and mood. The nature of the GlobalSurgBox is it allows trainees to take control of their own education. No longer do trainees need to sign up for dedicated scheduled time in a simulation center. They now have the flexibility of practice on their own terms. With our online curriculum and tutorials that we are designing and updating continuously, this becomes even easier to do.
Procedure[edit | edit source]
The GlobalSurgBox is a key component to preparing a trainee for effective and safe practice in the operating room. Before even stepping into an operating room, the GlobalSurgBox (and its associated website and mobile application) will be able to effectively deliver the knowledge base and milestones, as well as the surgical skills and techniques required for every learner. Even after a trainee has been able to operate on a patient, the GlobalSurgBox serves as a continued way to learn and improve on their clinical judgement and technical skills.
We envision the GlobalSurgBox being integrated in surgical curriculums all across the globe. In the next year, the GlobalSurgBox is going to be used in pilot sites in in Kenya, Rwanda, and the USA. We have already committed to designing and implementing curricula for general surgery residency training programs in Rwanda (4 year training program), Kenya (5 year program), and the Colorado USA (7 year program). We are also actively designing a curricula for medical students at the University of Global Health Equity in Rwanda starting in January 2022.
To ensure equitable access to these resources, and allowing anyone to use this curriculum, we have created a website (https://globalsurgbox.com/) that includes multiple aspects of the surgical simulator:
- Step-by-step instructions on how to construct the simulator.
- Explanations of each part of the simulator and how they can be used for simulation.
- Videos of all modules to be performed, including materials needed, setup of the module, the procedures of the simulation, and additional tips and tricks for success.
We have created many modules already, including knot tying (one-hand, two-handed), basic suturing skills, end-to-side vascular anastomosis, with many others on the way. Each module will include expert videos which give practical and clinical advice pertinent to each operative skill. For example, if a participant is practicing a CABG anastomosis, there will be a video detailing how to perform the anastomosis, and additionally a video explaining common pitfalls in the operating room and offer examples of situations where the operative technique might need to deviate from the typical technique taught in the video.
We are also creating an mobile application which will have the following uses:
- Integration of knowledge and clinical judgement quizzes within the app. This will ensure that aspects of surgical procedures including anatomical knowledge and clinical decision making are also included.
- Allow users to videotape themselves practising a particular skill and upload to an app, which they can either review in the future or send to specified mentors through the app.
- Allow mentors to assess learners with assessment tools integrated within the app, as well as give feedback through the app. The advantage of using a mobile or web application means that asynchronous learning can happen, increasing the chances for success.
- Allow inter-facility and international competitions between different trainees to increase use.
Self-Assessment[edit | edit source]
Self-assessment and independent training is a key part of the GlobalSurgBox. We plan to measure the success of our simulation training using competency based milestones as well as the Entrustable Professional Activities (EPAs) framework. Competency based milestones have been a cornerstone of medical and surgical education for decades. However, there has been some discussion that competencies in isolation are too theoretical and may not transplate to clinical practice, which is especially a concern in surgical training. Therefore, we plan to also use EPAs as a tool to ensures translation of these competencies into actual pratice and performance. The EPA framework is currently being integrated into many training programs including surgical training programs (Nuts and Bolts of Entrustable Professional Activities - nih.gov).
We are in the process of creating full curricula with many integrated modules. All of our modules will be standardized with the following:
- knowledge transfer
- knowledge assessments
- skills transfer through resource guides and instructional videos to ensure proper technique is being taught and reinforced
- skills assessment through direct feedback from instructors as well as asynchronous feedback through a future web application
Website and web application: To ensure easy access to training modules, we plan to create resources that are freely available to all trainees. This will be done through a website (www.globalsurgbox.com) and in the future, with grant support, an integrated a web application. The website that we have developed is the first stage towards standardizing these resources. The smartphone application we are developing will include the following features to allow for comprehensive self assessment: (1) ability for user to record videos of them performing the skill (2) complete quizzes on anatomy and clinical decision making, (3) compete with other trainees across the globe, (4) “test” the integrity and competence of certain skills (5) allow for learners to be assigned a surgical mentor, (6) allow mentors to objectively assess learners through standardized forms, as well as provide space for specific feedback and comments corresponding to the individual mentee videos.
Recording user videos: Our phone application will not only include teaching modules, but will also include the ability of the user to record videos of themselves performing each exercise. Our simulator includes a landing platform/phone stand to place a cell phone of any size, such that exercises being performed on the wood simulation platform can be recorded. These recordings will allow for mentors from any country or setting to be able to give feedback on technique and set up. In addition, users can watch their videos over time and visually assess their progress and development, compared to the standardized video.
User Quizzes: We will integrate quizzes on anatomical knowledge and clinical decision making for each module that is taught. These will be designed in conjunction with surgical educators and mentors and will have varying levels of difficulty depending on the users training.
Compete with other trainees: This integrated feature of the app will not only allow trainees to gauge their learning against peers in a unique and asynchronous way, but will improve the use of the surgical simulator and motivate the user to continue practicing and developing their skills. There will be an integrated “leader board” and competitions on speed, quality, and different techniques that users can participate in by submitting individual videos. Over time, this competition feature will be used to select trainees to qualify for the in person surgical skills competition held at a yearly College of Surgeons of East, Central and Southern Africa (COSECSA) conference.
Self assessment of skill completion and integrity: On both the website and the phone application, there will be instructions on how to ensure you have mastered a certain skill, separate from mentorship feedback. For example, a step by step guide for a water submersion test to ensure the practiced anastomosis lacks holes or gaps.
Surgical mentorship: Each set of learners will be assigned a surgical mentor, who will have access to any video that the user wishes to share. The opportunity for mentorship in an asynchronous and non-local fashion is a major component of the scalability of surgical simulation within low- and middle-income countries. Mentors will also keep track of milestones that the learners need to achieve at specific time points.
Mentor feedback: Mentors will assess learners for competence in being able to perform a specific task or technical skill through a standardized checklist for each module. Feedback can be provided through the app by general comments on each video sent, or direct feedback at set time periods in the video for more specific and detailed observations.
We believe that the integrated feedback will encourage autonomy in the operating room and accelerate the learning of our trainees. In addition, the platform for providing feedback allows for scalability and asynchronous teaching. These factors help to ensure the sustainability and practicality of this simulation tool across various resource settings.
Innovation[edit | edit source]
GlobalSurgBox is a great solution for teaching operating room surgical skills because of its low cost, adaptability and portability. Other surgical skill simulators tend to be available for use at the hospital or need a guided teacher, which makes this traditional approach harder for most trainees, and more so for those in LMICs. In addition, most of the commercially available simulators use parts that are difficult and expensive to replenish, such as animal tissue or silicone. Our model prioritized the use of universally available materials such as cotton, rubber and wood, all of which can be purchased in bulk to drive down the cost per box to less than $25. Moreover, the durability and portability of a toolbox takes into consideration many of the challenges of setting up a traditional simulation lab. We have consulted with our colleagues in Kenya and Rwanda to ensure the nature of their needs in simulation.
We envision the GlobalSurgBox to become a key portion of all surgical training curricula, whether it be medical student education, or residency and fellowship training. Therefore, we have thoughtfully considered multiple training curricula in order to create the most comprehensive and useful modules to be used with the GlobalSurgBox. In this manner, we ensure that the GlobalSurgBox can be easily integrated into major training programs around the world at scale, and it will be seen as a significant enhancement to existing platforms rather than a complete switch of curricula. This includes the COSECSA (College of Surgeons of East, Central and Southern Africa) overall curriculum, the ACGME (Accreditation Council for Graduate Medical Education) Surgical milestones, as well as the Basic Surgical Skills Course and Core Surgical Training by the RCSI (Royal College of Surgeons in Ireland) and RCSEd (Royal College of Surgeons of Edinburgh).
Evolution of the GlobalSurgBox[edit | edit source]
The GlobalSurgBox is a confluence of several ideas surrounding optimization for the common limitations of both surgical simulation and global surgical education. The original design was inspired by a simulator that fit in a shoebox. In an effort to make the simulator completely portable, we changed the design to be housed within a toolbox, which not only enabled ease of transport but also the ability to store and organize extra instruments and material in the different compartments. From there, we designed modules that were suited to each level of trainee and found cost-effective materials for each module. All the materials for the modules were tested and we continue to work with our colleagues and users to update them to be more affordable, user friendly, and as close to the real deal as possible.
We completed initial testing of the surgical simulator in the US with surgical residents at the University of Colorado Hospital. 30 residents used the simulator prior to filling out a voluntary, anonymous survey asking if the GlobalSurgBox was a realistic replica of the operating room. All 30 residents stated that the GlobalSurgBox was helpful in preparing them for the operating room. Furthermore, residents stated that it reduced multiple barriers to simulation, including lack of convenient access and cost. Finally, all residents stated that the GlobalSurgBox encouraged practice outside of the operating room. These results are encouraging as they lead us to believe that this simulator is valuable to surgical trainees.
We further tested the GlobalSurgBox in Kenya to prove our hypothesis that this simulator would be helpful not only in a high-resource setting in the US, but also in a lower resource setting. 27 learners, including medical students, medical officers, residents, and cardiothoracic surgery fellows used the trainer with similar results. Many of the participants also commented on the feasibility of replacing many of the GlobalSurgBox components with locally accessible materials they had easily available. This strong positive response is affirmative of the usefulness of the GlobalSurgBox and shows it is not limited by resource setting or level of the learner. We then finally tested the GlobalSurgBox in Rwanda, which led to new ideas of integration into training curricula and the use of competency based training and Entrustable Professional Activities (EPAs).
For the next phase of this project, we plan to formalize curricula for all settings, which will include full modules for each level of learner. We will create a formal curriculum for general surgery residents, as well as medical students, with milestones to achieve for each postgraduate year. Every module will include an instructional video, targets and goals to achieve, as well as specific assessment forms which will include handling of tissue and instruments, efficiency of movement, surgical technique, and time to successful completion of exercise.
Adoption in resource-constrained settings[edit | edit source]

We plan for our simulator to reach a large population of surgical trainees in LMICs. We already have plans for integration into Kenya, Rwanda, and COSECSA programs. We anticipate that this will then lead to further implementation in more settings around the world.
One of our partner sites is Tenwek Hospital in Kenya, which is one of the College of Surgeons of East, Central, and Southern Africa’s (COSECSA) approved surgical training programs. COSECSA is the largest surgical training institution in Africa, operating in 14 countries, and fosters postgraduate education. COSECA provides a common surgical training program and examination. The implementation of the GlobalSurgBox will begin in Tenwek, and with assistance from Tenwek will grow and be adapted for other COSECA institutions. In order to facilitate continued use and construction of the box, detailed instructions on how to build it, as well as a variety of approved materials are listed on our website. Many materials can be purchased locally, or will be readily available to ship from the United States if requested on the website. We plan to recreate the GlobalSurgBox in Kenya and Rwanda using materials only found in the respective countries, to ensure that all materials are easily able to be replenished, ultimately ensuring sustainability of the project. We will facilitate this adaptation to locally sourced materials by issuing a rewarded call for ideas to LMIC surgical trainees. An example of this call for ideas is depicted in Figure 3.
These trainers will also be used for training undergraduate medical students and interns in Rwanda through the University of Global Health Equity (UGHE), where it is being integrated into the Entrustable Professional Activity directed, competency-based surgical curriculum of the six and a half-year, joint Bachelor of Medicine, Bachelor of Surgery/Master of Science in Global Health Delivery (MBBS/MGHD) degrees. GlobalSurgBox is positioned as an important aspect of the surgical simulation program aimed at preparing students for independent surgical practice as general practitioners. The trainers are being incorporated into Entrustable Professional Activity assessments, and clinical training. In the first instance, 30 medical students in Rwanda will be trained per year using the simulators and the simulation modules in the pilot phase (90 students). This is a long term process/partnership that will allow us to track the effectiveness of the GlobalSurgBox in preparation of undergraduates for the transition to operative general practice over the space of 3 years. UGHE’s Center for Equity in Global Surgery is also committed to scaling this intervention as Continuing Medical Education for Rwandan practitioners.
Another solution to ensure all users can access the GlobalSurgBox is integrating the boxes into a "simulation library" in resource constrained areas, where students can check out boxes for a certain period of time and return them, similar to checking out library books or other resources.
Users[edit | edit source]
Our potential users are any student of surgery, whether it be medical students, residents, fellows, general practitioners, or faculty who wish to train these students. We conducted a recent survey in Kenya and respondents (n=27) all agreed with the statement that surgical simulation is an important adjunct to their training, however only 50% had access to current simulators, typically through their training program. Of those with access to simulators, 76% reported barriers to current use such as lack of time or convenient access. The ease of transport, setup, and material replenishment of the GlobalSurgBox make it an optimal solution to this problem.
In Rwanda, up to 90% of c-sections are performed by general practitioners who have only had medical school training, and are in independent, unsupervised surgical practice at District hospital level. Students must deliberately prepare for this transition, and we have tailored the design of our surgical training modules to help.
Reproducibility[edit | edit source]

Based on our survey of Kenyan participants we found that simulators currently accessible to trainees were those provided by the training program. These are typically focused on knot tying, skin closure, or laparoscopic skills. The cost of these models would be prohibitive for an individual to purchase, and they are not readily accessible, as they require access to a simulation center in the hospital. Cost was at the forefront of our mind while creating the GlobalSurgBox.
Our model prioritizes the use of universally available materials which drives down the cost per box. One barrier we found with previous surgical simulators is that many of the materials needed are not easy to replace, making it difficult for users to continue with their simulation. Therefore, when we created the GlobalSurgBox, we emphasized the need to source materials that are easily replaceable as well. All of the materials can be found in local stores, maximizing the use of the simulator.
Moreover, the durability and portability of a toolbox takes into consideration many of the challenges of setting up a traditional simulation lab, allowing a greatly increased ease and frequency of practice. Finally, the toolbox has a modular component which allows the skills taught to be modified based on the growing skills of the learner. The GlobalSurgBox can be used by a learner throughout the entire length of training, from medical student, resident, to surgical fellow.
In order to ensure easy handover we have created detailed videos and handouts available on our website that list materials needed for the simulator and step-by-step instructions for assembly. This will ensure that any participant could easily create their own GlobalSurgBox. Fig 4 shows an example of all the materials required to create a GlobalSurgBox, including their source such that users are able to purchase them easily.
How can anyone around the world access the GlobalSurgBox?[edit | edit source]
With the creation of our website and partnership with many educational institutions in Africa, anyone in the world can purchase a box through the website or build it themselves with locally-sourced materials using our detailed creation instructions. By providing a freely available resource for anyone to create and improve their own simulator, we reduce a major aspect of gatekeeping in surgical simulation.
This website also improves the scalability of educational resources, another significant barrier to surgical education in LMICs. The phone application that we are currently developing will build on this. As a free resource where simulation modules and examples, instructional videos, quizzes, and free mentorship will be housed it will allow any student, trainee, or educational program in any location to engage with the content and ultimately make surgical training more accessible. The capstone of reducing these barriers is the inclusion of mentorship directly into the application. By enabling trainees to receive guidance from surgical educators from around the globe, the often severe limitation of local access to mentorship in LMICs can be reduced. Trainees can share their simulations, receive constructive feedback on improving their technical skills, and make the most of their training time in the OR by deploying and honing well-practiced skills.
Additional Modules[edit | edit source]
Medical Student Module[edit | edit source]

Surgical square knot tying is a basic skill of surgical practice. As such, it is practiced routinely throughout the course of surgical procedures. Learners will be able to demonstrate the translation of this simulation into clinically valid skills each and every time they scrub into a surgical procedure. They will also be able to directly apply their knot tying ability as a core requirement of progressing to the next and more technically challenging simulations.
This is a simple module, but a very important one for early and beginning trainees.
Surgical Resident Module[edit | edit source]
Suture skills are another fundamental skill of medical students, residents and surgeons. However, this often requires a steep learning curve and lots of practice. Simulators such as artificial skin pads are available for trainees to learn, however, they are often expensive and not replenishable locally for users in low and middle income countries.
Suture skills with the GlobalSurgBox allow for adaptability and growth with the learner, but with a low cost.
Surgical Fellow Module[edit | edit source]
Video coming soon.
Through demonstration of the fundamentals of vessel anastomosis technique, learners will be able to understand the essential components of a secure and patent anastomosis. These include both an end-to-end anastomosis and an end-to-side anastomosis. They will then be able to practice the stepwise completion of each anastomosis using the vessel anastomosis simulator.
This opportunity for physical skill performance and repetition will allow learners to gain confidence and proficiency in the proper execution of this skill. Once developed, surgical trainees will be able to apply this skill in the operating room, where practice and experience will spare patients undue morbidity that could result from initial learning taking place in the operating room.
The value of GlobalSurgBox is not in each individual module alone, but the combination of these modules in one small box. Skill training and OR confidence is gained for a low cost, through simulation that progresses alongside the developing learner.
References[edit | edit source]
- de Montbrun SL, Macrae H. Simulation in surgical education. Clin Colon Rectal Surg. 2012 Sep;25(3):156-65. doi: 10.1055/s-0032-1322553. PMID: 23997671; PMCID: PMC3577578.
- Feins RH, Burkhart HM, Conte JV, Coore DN, Fann JI, Hicks GL Jr, Nesbitt JC, Ramphal PS, Schiro SE, Shen KR, Sridhar A, Stewart PW, Walker JD, Mokadam NA. Simulation-Based Training in Cardiac Surgery. Ann Thorac Surg. 2017 Jan;103(1):312-321. doi: 10.1016/j.athoracsur.2016.06.062. Epub 2016 Aug 25. PMID: 27570162.
- Tansley G, Bailey JG, Gu Y, et al. Efficacy of Surgical Simulation Training in a LowIncome Country. World J Surg. 2016;40(11):2643-2649.
- Livingston et al. Development of a simulation and skills centre in East Africa: a Rwandan-Canadian partnership. Pan African Medical Journal. 2014. 17:315.
- McIntosh, Cate; Macario, Alex; Flanagan, Brendan; Gaba, David M Simulation: What does it really cost?, Simulation in Healthcare: The Journal of the Society for Simulation in Healthcare: Summer 2006 - Volume 1 - Issue 2 - p 109
- Henry B, Clark P, Sudan R. Cost and logistics of implementing a tissue-based American College of Surgeons/Association of Program Directors in Surgery surgical skills curriculum for general surgery residents of all clinical years. Am J Surg. 2014 Feb;207(2):201-8. doi: 10.1016/j.amjsurg.2013.08.025. Epub 2013 Oct 23. PMID: 24239527.
- Durko A, Thuijs D, Mahtab E, Bekkers J. How to construct and use a low-fidelity coronary anastomosis simulator. Multimed Man Cardiothorac Surg. 2019; doi:10.1510/mmcts.2019.006.
- Kelly J, Iyengar A, Patrick W, Helmers M, Smood B, Han J. Cardiac surgery simulation - Part 1: Basic Surgical Skills. Multimed Man Cardiothorac Surg. 2020; doi:10.1510/mmcts.2020.073.
- Moscarelli M, Di Bari N, Bonifazi R, et al. How to assemble a low-fidelity simulator for minimally invasive mitral valve surgery. Multimed Man Cardiothorac Surg. 2019; doi:10.1510/mmcts.2019.014.