Background
Dialysis in the desert
In remote Australian communities, Aboriginal Australians suffer kidney failure at a rate that approaches 10 times the national average. Transplants are rare and frequent dialysis is usually prescribed. Many dialysis patients are elderly and senior members of these remote communities. In an effort to improve the social health of both communities and patients, there has been a recent push to increase dialysis services within remote communities and clinics (Devitt and McMasters, 1998, pg.67). Unfortunately, many of these communities are in arid regions, which means town water tends to be warm where it comes out of the tap.
Remote water temperature
In remote communities, town water is typically raised from the aquifer, then treated and stored in large tanks, often on the top of a hill in the sun. Tank water is piped over-land to various points including each remote clinic, where it may be stored in a smaller clinic’s tank. In summer, air temperatures may approach 50C. By the time the water gets to a clinic it is usually quite warm. Dialysis water pre-treatment depends on small RO systems, which tend to lose effectiveness as the water temperature rises, eventually posting errors and shutting down with water temps around 35C.
The RO systems are designed to fail safely when the incoming water temperature is too high. However, any equipment failure may cause dialysis treatments to be cancelled. Since patients need dialysis treatments on alternating days, a delay of more than one day means transport of the patient to a regional centre (usually Alice Springs) for treatment. This is both expensive and detrimental to the health and wellbeing of the patients. In short, the consequences of missed dialysis are significant from a patient wellbeing and public-health perspective.
Project details
Technical requirements
To provide a source of cool water (below 35 C) to remote clinics at a rate of 1L/min per dialysis machine.
Specification

A remote community water supply may reach temperatures greater than 45 C. An RO machine will alarm when its supply temperature is greater than 37 C. An effective pre-cooling device would be one that could reliably take 10-15 degrees C off the supply water temperature at a rate of about 1 L/min. This is equivalent to about 1.2 kW of heat that needs to be extracted from the incoming water.
One of the main challenges of this project involves finding a suitable place and means to sink the heat that is extracted from the water. It is difficult to sink the heat into the outside air, as it can be much hotter than the supply water. Such techniques have been attempted by using chiller packages that operate outside a dialysis clinic and attempt to pump heat from the water directly into the even hotter air. This has been shown to be unreliable due to solar loading and other challenges of heat transfer.
Air conditioning cooling capacity
One approach is to sink the heat into the room's inside air and allow the air-conditioning systems to pump the heat outside. The main advantage of this approach is that the air represents a thermal store that can quickly absorb the heat from the water before it is slowly pumped out by its air-conditioners. The second advantage is that there are usually more than one split-system air-conditioning unit installed in each clinic, providing ample capacity to pump heat from the inside air to the outside environment. A typical split-system air-conditioner has a cooling capacity of about 8 kW. This is more than six times what is required to pump out the heat required to run a single dialysis chair on a hot day.
Existing solutions
Various informal methods have been attempted, such as running hose through a chest-freezer, draping tanks with wet cloth, storing water in a tank inside the clinic. None of these solutions have been engineered - they are mostly guesswork. At present, sites have purchased chiller packages - these are worth $8-10K each, are heavy, are not that effective at higher temperatures and are prone to failure.
Design preferences
- A good solution to this problem would be inexpensive, lightweight, effective, reliable and robust for us in remote sites.
- As maintenance is difficult at a remote site, a good design would be reliable and low-maintenance and/or usermaintainable
- Another approach to maintenance is to make the device lightweight and portable, such that it could easily be loaded by a single person into the cabin or tray of a 4WD and installed with a minimum of technical expertise.
- A good design would be able to be used together with any other cooling system without having to reconfigure the plumbing of the equipment or building.
Online cooling
First prototype



We have worked on the simplest possible concepts for cooling water for dialysis. At present, we have shown that water can be cooled sufficiently by running it through a simple heat-exchanger coil, while using a ~100 W household fan to blow air through its fins.
Measured Steady State Temperature Changes
- Example: Input water temp 46 C, Output temp 28 C, 1L/min = 1.2 kW
- Example: Input water temp 36 C, Output temp 28 C, 1L/min = 0.7 kW
By approximating the behaviour of this cooling system, we can estimate cooling capacity at 0.07 kW per degree C removed at 1.0 L/min flow-rate.
Physical dimensions
- Total size including extended surface matrix = 0.7 x 0.46 x 0.60 m
- Approximately 40 m of 7.7 mm OD, 6.7 mm ID pipe. About 1.5 L total fluid capacity.
Material costs
- Heat exchanger (new) about $300-$400
- Case and hardware ($100-$200)
- Labour: approx 10 hours to assemble from pre-cut sheets and parts.
Second prototype
The second protoype has been built using a new heat exchanger and high-pressure fluid couplings so that the unit can tolerate mains pressure water. It is now ready to be tested.
The fluid couplings are dimensioned to take 1.25 inch fluid connections.
Next steps
- The current prototype is made from junk parts and seems very effective, but is bulky. It would be nice to calculate exactly the efficiencies of various off-the-shelf fluid-air heat exchangers and optimise for smaller/lighter/cheaper etc.
- The design is based around a single-treatment at 1.0 L/min. In most clinics, more than one treatment may be operating at any time - it may be that a single design can cool enough water for more than one machine, or it may be simpler to develop one cooler per dialysis chair. This may be limited by plumbing and space arrangements in each clinic.
Other potential solutions
Offline cooling/storage

Some stakeholders have suggested pre-cooling an indoor tank full of water for dialysis, to save cooling it on-demand. This may be done to take advantage of the cooler night-time weather for cooling water, then storing it until the morning for treatments. By using a heat-exchanger similar to that described for the online approach, water could be circulated through a storage tank and a heat exchanger device over a 12 hour period and the heat could be dumped into the building's inside air and allowing the air-conditioner to pump it outside.
What shape and size of water storage vessel in an airconditioned room can chill 300 L of water by 10 C in 12 hours overnight?
The main design challenges with this approach are as follows:
- A large tank needs to be constructed and installed within the building.
- The entire volume of the tank needs to be cooled for any of it to be usable.
Water used at 1.0 L/min for five hours is 300 L. Rather than have one tank per chair, it makes sense to cool all the required water for all dialysis chairs. To run two chairs requires 600 L of water for treatment, plus extra water for cleaning cycles before and after each treatment. If we aim for a minimum of 1000 L tank capacity for two chairs (2000 L capacity for a four-chair clinic), then we must sink a large amount of heat overnight.
With a heat exchanger operating at twice the capacity of our tested online prototype, it is possible to cool sufficient water and store it in a tank overnight. Generally speaking, it would appear that the optimal combination is a small tank and a large, efficient heat exchanger.
- Sample gallery
-
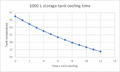
Temperature drop in degrees C overnight using a heat exchanger similar to the prototypes shown and a 1kL storage tank.
-
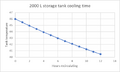
Temperature drop using a similar heat exchanger and a larger tank.)
-
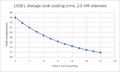
Temperature drop using a larger heat exchanger and a small tank.
-
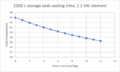
Temperature drop using a larger heat exchanger and a large tank.




What is the optimal capacity of offline storage volume and heat transfer capacity (kW) to provide enough cooled water in 12 hours overnight for two dialysis treatment chairs?
Active cooling
For mobile dialysis, the air-conditioning units are small and cannot be expected to handle the extra load of water cooling. Some stakeholders have suggested Peltier modules or similar electronic heat-pump may be developed for this purpose. One mobile unit has a "dispatch hatch" with dimensions 1200 mm side and 500 mm high with a door that hinges upward, which may be used to pump heat from inside a mobile dialysis clinic truck-body.
What is the simplest active heat-pump that can be built to transfer heat from water to air at 1.2 kW per dialysis machine, through a small opening in a vehicle?
Heat collection using phase-change material
There has been recent research in both the medical-device field [1] and in building-temperature management [2] regarding the use of phase-change material or salts as a combination of temperature-control and energy-storage. This type of project is probably the right kind of size and scale for this kind of application.
What type and quantity of PCM is needed to extract and store at least six kWh of heat from a potable water supply delivered at 1.0 L/min?
Appropriately sized packs of PCM could be exchanged and cooled offline or offsite.
Future work
Where else in the world would this be useful, and who else has solved this problem and in what ways? Is this technology useful in other parts of the world? This problem exists in about 10-20 remote communities in Central Australia, and there are rumours of a similar problem in South Australia. There may be similar problems in arid/hot regions of other countries that suffer chronic kidney failure (Sahara desert, perhaps?). There is more to be said about this later.
References
Contact details
biomedkitchen@gmail.com